
ACOs Are Great On Paper, But Is That Enough?
When it comes to accountable care and other shared savings organizations, CIOs support the overall premise, but when it comes to application, it’s often a different story. In the August healthsystemCIO.com Snap Survey, nearly half (47 percent) of respondents said their organization is participating in an ACO and 13 percent are in the process of joining one, but CIOs still aren’t sure if the model will prove to be successful.
“The goal is great, but system integration is difficult,” said one respondent.
When asked about the most significant challenges, 40 percent of CIOs cited interoperability/integration, while 20 percent pointed to governance/leadership. One CIO said the process of obtaining data from community physicians is “challenging,” adding that “‘interoperability’ is a gleam in the eye of the beholder.”
According to the survey, a little more than half of CIOs said the level of integration between hospitals and physician practices is “low,” with 26 percent characterizing it as “moderate.”
And it isn’t just data exchange with providers that poses a barrier, but payers as well, noted one CIO. “The challenge of trying to normalize and integrate a wide variety of data from differing payers has been somewhat overwhelming, leaving little time or resource to address integration between the practices and the ACO.”
As far as whether they believe accountable care organizations will be successful, CIOs are divided. Some express concerns about the burden of cost being placed on hospitals, some are optimistic that the model will improve through shared best practices, and some are unsure.
(SnapSurveys are answered by the healthsystemCIO.com CIO Advisory Panel. To go directly to a full-size version of any individual chart, click on that chart.)
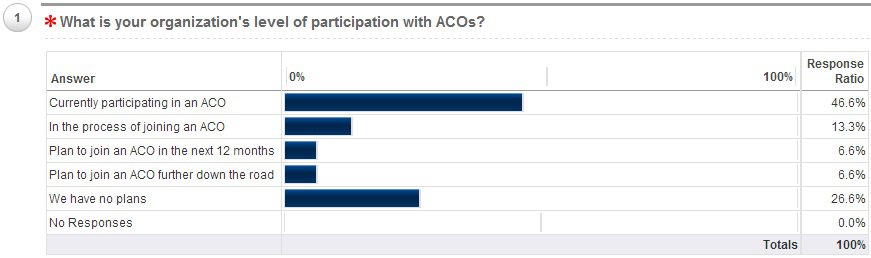
1. What is your organization’s level of participation with ACOs?
Currently participating in an ACO
- We are in year two of a Medicare shared savings ACO.
- We are currently involved in shared savings arrangement with two commercial payers, along with our MSSP.
In the process of joining an ACO
Plan to join an ACO in the next 12 months
Plan to join an ACO further down the road
We have no plans
- We lead the market in lowest cost of care everywhere we are at. To join an ACO would be allowing the others to compete at our level, and that is just not going to happen.
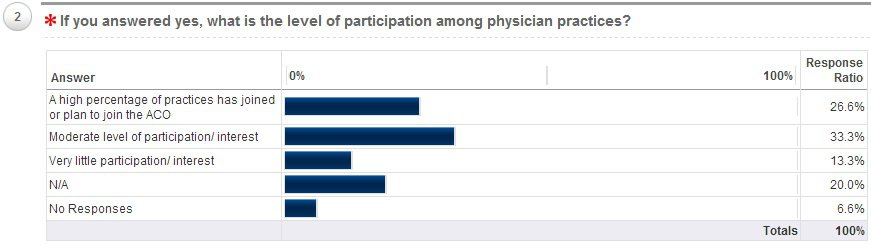
2. If you answered yes, what is the level of participation among physician practices?
A high percentage of practices has joined or plan to join the ACO
- All of our physicians (we are a large IDN) are participants.
Moderate level of participation/interest
Very little participation/interest
N/A

3. Are both hospital and physician practice leaders represented on the governance board?
Yes, we have both hospital and physician leaders
No, only hospital leaders
No, only physician leaders
I’m not sure
N/A
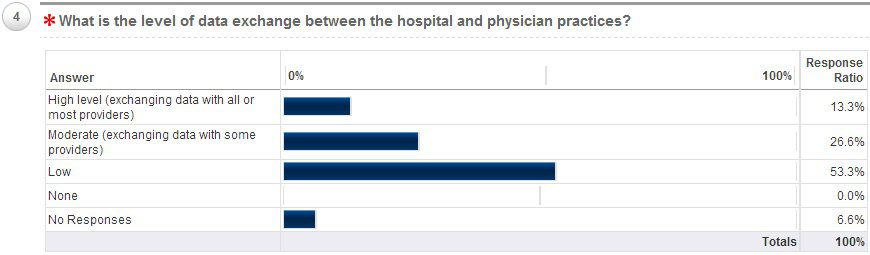
4. What is the level of data exchange between the hospital and physician practices?
High level (exchanging data with all or most providers)
Moderate (exchanging data with some providers)
Low
None

5. What is the most significant challenge in building and maintaining a successful ACO?
Involvement from physician practices
Interoperability/integrating multiple EHRs
- Our current ACO includes only members of our group practice, all on the same instance of our EMR. Accessing data from community network partners is challenging indeed with spending millions on an HIE topology. At present, “interoperability” is a gleam in the eye of the beholder (maybe a stye!).
- The interoperability challenge is not just between providers, but also payers. The challenge of trying to normalize and integrate a wide variety of data from differing payers has been somewhat overwhelming, leaving little time or resource to address integration between the practices and the ACO, although we are exchanging data with our regional HIE.
Ability to perform high-level analytics
Governance/leadership
- I was part of another organization that started an ACO. It was shut down as they could not figure out how to run it where all benefitted. I personally think this is a poorly conceived direction and is not going to survive. Think about the early to mid 90’s with HMOs and all the provider systems that were going to run their own.
Patient engagement
Other
6. Do you believe ACOs are or can be successful in improving the quality of care and reducing costs? Why or why not?
- If they reduce cost and improve quality, yes.
- Yes, the goal is great but system integration is difficult.
- No, the cost will continue to rise.
- No, it is cost shifting to the hospitals.
- Not enough room to answer this question.
- No. Direct contracting with provider organizations will prevail.
- Relatively, yes. It is soon to be a forced care model.
- Unknown.
- The incentives are aligned to make this successful.
- Yes, as we will have best practices/more learning.


Share Your Thoughts
You must be logged in to post a comment.